When Trauma Therapy Feels Unsafe: How DBT Skills Support Ethical, Sustainable EMDR Work
May 27, 2026
The Quiet Ethical Panic Many Trauma Therapists Carry
There's a particular kind of dread that shows up on Sunday evenings. You're not thinking about your whole caseload. You're thinking about one client. The one who texted from a parking lot at 11pm last week. The one who cycles through crises so reliably you've started bracing before every session. The one you genuinely don't know how to hold.
Most therapists don't say this out loud. But the internal monologue is real, and it sounds something like: Do I have enough structure to safely hold this case? Am I practicing ethically with this level of risk?

That question isn't a sign of incompetence. It's actually a sign of clinical integrity. You're asking because you care. Because somewhere in your training, you absorbed the weight of what it means to sit with someone who is genuinely unsafe, and you take that seriously. That's not a problem. That's an appropriate professional concern.
What is a problem is when that concern has nowhere to go. When you're improvising session to session, managing each crisis as it comes, and quietly wondering if there's a better way. There is. And it doesn't require you to become a DBT specialist or overhaul your entire practice. It requires something more practical than that: a framework.
Why High-Risk Trauma Cases Push Therapists to the Edge
Let's be honest about what high-acuity trauma work actually looks like in a real caseload. We're talking about clients with chronic suicidal ideation who have been hospitalized multiple times and are still struggling. Clients who self-harm not because they want to die but because it's the only thing that works when the nervous system goes haywire. Clients with dissociative presentations who slip out of contact mid-session. Clients with attachment histories are so chaotic that the therapeutic relationship itself becomes a trigger.
These presentations are not rare. They're the population that tends to find their way into trauma therapy precisely because standard approaches haven't worked. And there's a significant mismatch between what those clients need and what most graduate programs actually trained you to do.
Insight-oriented approaches assume the client can reflect, integrate, and metabolize. Exploratory therapy assumes relative stability. But clients with chronic suicidality, active self-harm, and severe dissociation often can't access those capacities reliably. They don't need more exploration. They need tools. Concrete, learnable, repeatable skills they can use when the nervous system is in full revolt.
Without those tools on your side of the room too, you're working harder than you need to. And over time, that has a cost.
How Lack of Structure Increases Risk and Burnout
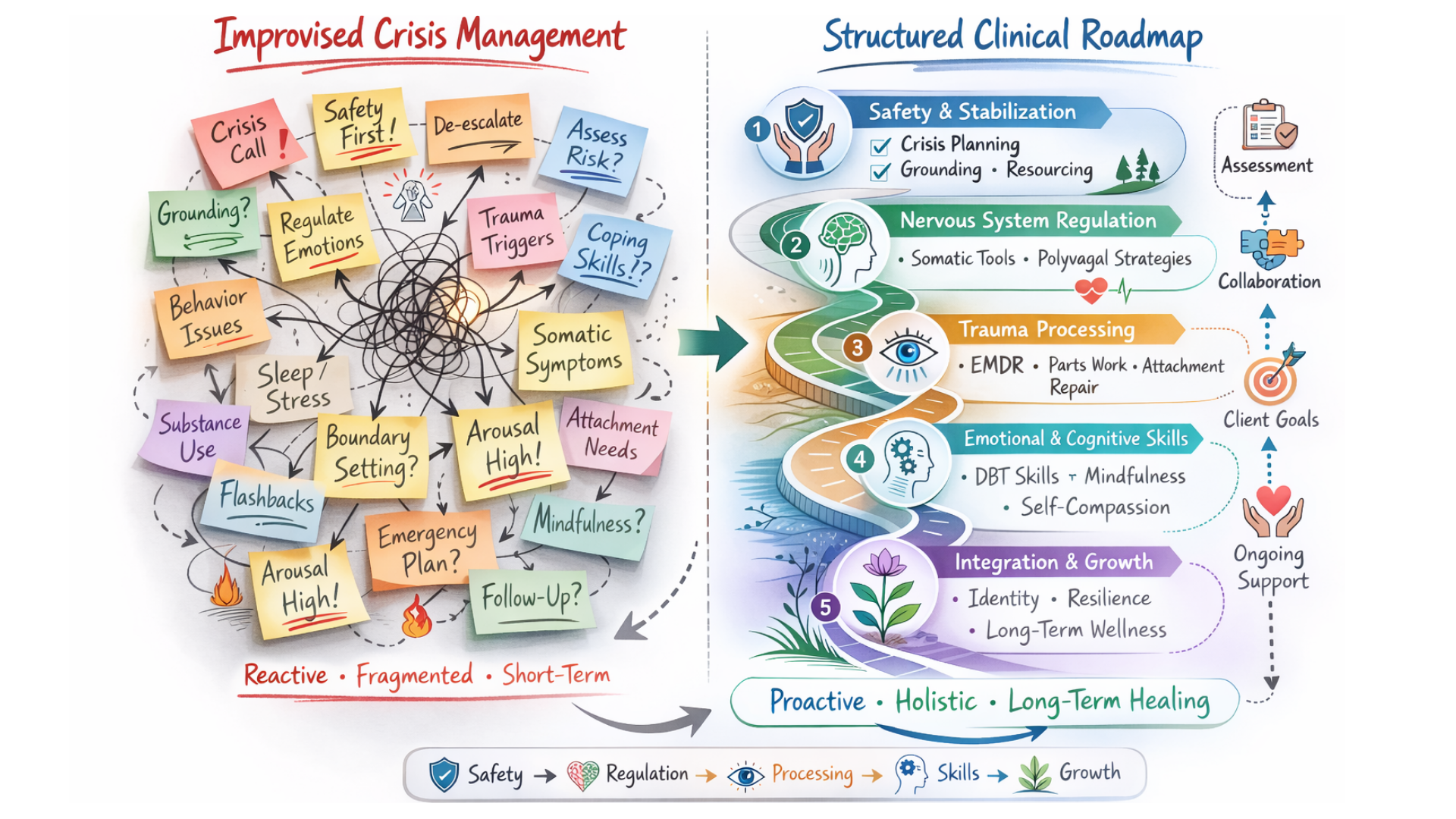
Here's something the research confirms that most therapists already feel in their bodies: working without a roadmap is exhausting. Not just emotionally. Physiologically. When you don't have a clear framework for what to do when a client destabilizes, your nervous system starts doing triage in real time, every session. That's not a clinical skill. That's hypervigilance.
A Simple Practice survey of over 1,000 therapists found that 52% reported burnout in the past 12 months, with 33% citing increased client acuity as a primary driver. Critically, 73% of burned-out therapists said they now hesitate to take on severe or acute clients. That's not a personal failing. That's a rational response to an unsustainable workload without adequate structure.
The pattern tends to look like this: you're constantly "talking clients down" without a clear clinical plan. You spend the last ten minutes of every session firefighting. You leave work not depleted from meaningful connection but depleted from sustained vigilance. The clinical term for what accumulates is compassion fatigue. The lived experience is that you dread certain clients, and then feel guilty about dreading them.
A systematic review published in Psychotherapy Research found that clinical complexity and lack of adequate training were among the most commonly cited contributors to therapist burnout. Not the clients themselves. The mismatch between what therapists were asked to hold and the skills they had to hold it.
That's a fixable problem.
DBT Skills as Ethical Clinical Structure
Dialectical Behavior Therapy was specifically designed for this population. Not high-functioning clients in existential distress. Clients with borderline personality disorder, chronic suicidality, self-harm behaviors, and the kind of emotional dysregulation that makes standard therapeutic approaches functionally useless. Marsha Linehan built DBT because existing treatments weren't working, and the result is one of the most structurally rigorous frameworks in the field.
But here's the thing that often gets lost: DBT isn't just good for your clients. It's good for you.
According to research reviewed by the APA, DBT therapists working with high-risk populations show lower rates of burnout than comparable therapists working without that framework. The consultation team structure, the clear treatment hierarchy, the predictable session focus: these aren't just clinical tools. They're sustainability mechanisms.
So what does DBT structure actually provide when you're working with high-risk trauma clients?
- A clear session hierarchy so you always know what to address first. Life-threatening behaviors before quality-of-life issues, always. That clarity alone reduces the cognitive load of every session significantly.
- Specific, evidence-based tools for self-harm and suicidality. Rather than improvising in the moment, you have behavioral chain analyses, diary cards, skills coaching, and a structured approach to crisis that doesn't rely on your intuition alone. The Behavioral Tech Institute outlines how DBT reduces psychiatric hospitalizations while simultaneously reducing suicidal behavior, partly because it gives clients tools to use in their own environments.
- A framework for informed consent that actually functions. When you have a skills-based framework, you can tell a client: here's what we're working on, here's why, and here's how we'll know when we're ready for the next phase. That transparency is clinically and ethically meaningful. It's also what the ethical standards for EMDR with complex trauma increasingly call for.
- Protection against the therapeutic drift that leads to burnout. When DBT therapists in one study were asked about using DBT skills in their own lives, over 75% reported daily use of mindfulness and emotion regulation skills. The framework becomes a resource, not just a clinical obligation.
The ethical question here matters: Is it ethical to keep working with a high-risk client if I don't feel confident I have the right skills?
The honest answer is that continuing without addressing the skills gap is the riskier ethical position. Your discomfort is accurate clinical data. It's telling you something needs to change, and the responsible response is to change it, not to push through and hope.

Where EMDR Fits: Safely Doing Deep Work with Structured Support
For therapists working with trauma, EMDR is often the goal. It's powerful, it's evidence-based, and for the right client at the right time, it can move things that years of talk therapy haven't touched. The challenge is that EMDR requires a nervous system stable enough to dual-track: processing past material while staying present in the room.
Many high-acuity clients aren't there yet. And when EMDR is attempted before a client is genuinely ready, it can destabilize rather than heal. This is one of the central concerns raised in EMDRIA's ethical standards for complex trauma treatment. Most basic EMDR training doesn't fully prepare clinicians for the complexity of dissociative or highly reactive presentations, and that gap creates real ethical risk.
DBT skills don't replace EMDR. They create the conditions that make EMDR safe. Here's how that looks in practice:
- undefined DBT's window of tolerance framework, combined with the polyvagal-informed understanding of nervous system readiness, gives you concrete criteria. Is the client using skills consistently? Are they maintaining safety between sessions? Is the therapeutic relationship stable enough to tolerate activation? These are assessable questions, not guesses.
- undefined When a client destabilizes mid-treatment, therapists often face a false binary: push through or give up. DBT gives you a third option. Returning to Phase 2 stabilization with active skills work isn't a failure or a retreat. It's good clinical sequencing. This connects directly to the somatic and stabilization-first principles that underpin ethical trauma treatment.
- undefined DBT's emphasis on behavioral specificity means you have measurable indicators for when re-engagement with trauma processing is appropriate. Not a gut feeling. Data from diary cards, session behavior, between-session functioning. That specificity protects both the client and you.
How does having a DBT framework actually reduce my risk as a clinician, not just my client's risk?
The answer is more direct than you might expect. A study examining DBT phone consultation and burnout found that therapists with more effective consultation teams and shared crisis response responsibilities had significantly lower burnout rates. More crisis contacts without structure predicted higher burnout. More crisis contacts with structure did not. The framework is protective. The isolation of improvising alone is what breaks people down.
Signs You Might Need More DBT in Your Practice
These aren't judgments. They're invitations. If several of these land, you already know what they're pointing toward.
- You find yourself dreading specific sessions the night before, and it's not because the work is hard, it's because you don't feel equipped.
- You spend significant session time talking clients down from a crisis without a clear clinical plan for what happens next.
- You're genuinely unsure when to push forward with trauma processing and when to pull back, so you default to one or the other without clear criteria.
- Your clients who struggle with self-harm seem stuck. You're managing the behavior without moving the underlying dysregulation.
- You've started avoiding certain referrals. High acuity clients who would have felt manageable earlier in your career now feel like risks you can't afford.
- After sessions with your most complex clients, you feel something beyond tired. You feel worn. That's compassion fatigue telling you the cost is unsustainable.
- You have general EMDR training but don't feel confident about when to initiate processing, pause it, or modify it for complex trauma presentations.
None of this means you're a bad therapist. It means you're a good therapist working at the edge of your current toolkit, and that edge is asking for something specific.

A Right-Sized Next Step: Foundational DBT Training for High-Acuity Work
Here's the question we should address directly before the CTA: Can I use DBT skills with clients in EMDR without completing full DBT certification?
Yes. And foundational DBT training is specifically designed for exactly this scenario. You don't need to become a DBT specialist or deliver a full DBT program to benefit enormously from the skills framework. What you need is enough working knowledge of the four DBT modules to integrate them meaningfully into the trauma and EMDR work you're already doing.
TTI's Intro to DBT: Skills Training for the Attuned Trauma Therapist is built for this. It's not a full certification program. It's targeted, foundational training designed for trauma therapists who work with complex, high-acuity presentations and need more structure, not more credentials.
The course covers all four DBT skills modules, specifically through the lens of trauma work and high-risk presentations:
- undefined as the foundation of dual awareness and trauma processing readiness
- undefined for managing acute crisis and self-harm urges without reinforcing avoidance
- undefined for the chronic dysregulation that underlies complex trauma presentations
- undefined for navigating the relational chaos that accompanies attachment-based trauma
Beyond the modules, the training addresses the specific high-risk scenarios that keep trauma therapists up at night: chronic suicidality, self-harm, dissociation, and the clinical decision-making framework for when to proceed with EMDR versus when to prioritize stabilization. For a deeper look at how EMDR and complex PTSD interact, TTI's resource on EMDR and Complex PTSD provides useful context on what foundational skills training makes possible.
This is confidence-building work. The kind of training that doesn't just add tools to your clinical bag, but fundamentally shifts how you feel walking into a difficult session. Structure is what makes high-acuity work sustainable. And sustainable care is ethical care.
Ethical Trauma Therapy Isn't Just About What You Do in the Room
It's about what you bring to the room. The frameworks you carry. The structure that holds you as much as it holds your clients. When you're improvising with complex trauma presentations, the risk doesn't stay on your client's side of the room. It accumulates in your body, your judgment, and eventually your capacity to keep doing this work at all.
DBT skills for high-risk clients aren't a specialty track for DBT therapists. They're a foundational element of ethical trauma therapy with anyone who presents at the complex end of the spectrum. And learning them at a foundational level doesn't require you to overhaul your practice. It requires a right-sized investment in the skills that change how the work feels.
If you've been sitting with the quiet ethical panic of not having enough structure for your most complex clients, that feeling is worth listening to. Not because something is wrong with you. Because something important is asking to be addressed.
The next step is straightforward.
Explore Intro to DBT: Skills Training for the Attuned Trauma Therapist at TTI.
Your clients need you to be sustainable. So do you.
References
Peer-Reviewed Journal Articles
Aarons, G. A., Fettes, D. L., Sommerfeld, D. H., & Palinkas, L. A. (2018). Predictors of burnout among community therapists in the sustainment phase of a system-driven implementation of multiple evidence-based practices in children's mental health. Professional Psychology: Research and Practice, 49(5), 327–336. https://pmc.ncbi.nlm.nih.gov/articles/PMC6157741/
Bhatt, M., & Bhatt, D. (2023). Ethical and legal aspects of trauma evaluation. Psychiatric Clinics of North America, 46(2), 413–424. https://pmc.ncbi.nlm.nih.gov/articles/PMC10316211/
Bourke, M., Carr, A., & Flynn, M. (2023). Clinicians' experience of collaboration in the treatment of suicidal clients within the Collaborative Assessment and Management of Suicidality framework. Frontiers in Psychology, 14, Article 1073698. https://pmc.ncbi.nlm.nih.gov/articles/PMC10227097/
Edelkott, N., Engstrom, D. W., Hernandez-Wolfe, P., & Gangsei, D. (2020). The COVID-19 era: How therapists can diminish burnout symptoms through self-care. Traumatology, 27(1), 6–14. https://pmc.ncbi.nlm.nih.gov/articles/PMC7602766/
Golynkina, K., & Ryle, A. (2017). Adapting dialectical behavior therapy for the treatment of dissociative identity disorder. European Journal of Psychotraumatology, 8(Suppl 1), Article 1298124. https://pmc.ncbi.nlm.nih.gov/articles/PMC5293140/
Harned, M. S., Wilks, C. R., Schmidt, S. C., & Coyle, T. N. (2021). Phone consultation and burnout among providers of dialectical behaviour therapy. Behavioural and Cognitive Psychotherapy, 50(1), 63–74. https://pubmed.ncbi.nlm.nih.gov/34490677/
Jobes, D. A., Chalker, S. A., & Ballard, E. D. (2024). The use of CAMS and DBT to effectively treat patients who are suicidal. Frontiers in Psychiatry, 15, Article 1354430. https://pmc.ncbi.nlm.nih.gov/articles/PMC11295142/
Kinman, G., McFall, M., & Rodriguez-Bailon, R. (2024). Effective burnout prevention strategies for counsellors and other therapists: A systematic review and meta-synthesis of qualitative studies. Counselling and Psychotherapy Research. Advance online publication. https://www.tandfonline.com/doi/full/10.1080/09515070.2024.2394767
Kotera, Y., Adhikari, P., & van Gordon, W. (2021). Burnout in professional psychotherapists: Relationships with self-compassion, work-life balance, and telepressure. International Journal of Environmental Research and Public Health, 18(10), Article 5308. https://pmc.ncbi.nlm.nih.gov/articles/PMC8156437/
Lynch, T. R., Trost, W. T., Salsman, N., & Linehan, M. M. (2010). Dialectical behavior therapy: Current indications and unique elements. Psychiatry (Edgmont), 7(9), 20–25. https://pmc.ncbi.nlm.nih.gov/articles/PMC2963469/
McCauley, E., Berk, M. S., Asarnow, J. R., Adrian, M., Cohen, J., Korslund, K., Avina, C., Hughes, J., Harned, M., Gallop, R., & Linehan, M. M. (2021). Efficacy of dialectical behavior therapy for adolescent self-harm and suicidal ideation: A systematic review and meta-analysis. JAMA Network Open, 4(8), Article e2121845. https://pmc.ncbi.nlm.nih.gov/articles/PMC8188531/
Rizvi, S. L., & Linehan, M. M. (2018). Dialectical behavior therapy as treatment for borderline personality disorder. Mental Health Clinician, 8(2), 62–67. https://pmc.ncbi.nlm.nih.gov/articles/PMC6007584/
Rzeszutek, M., Schier, K., & Gasik, R. (2022). Burnout and psychological wellbeing among psychotherapists: A systematic review. Frontiers in Psychology, 13, Article 942233. https://pmc.ncbi.nlm.nih.gov/articles/PMC9423708/
Web Resources
American Psychological Association Practice Research and Policy Staff. (2018, January 25). Research roundup: Burnout in mental health providers. APA Services. https://www.apaservices.org/practice/update/2018/01-25/mental-health-providers
Behavioral Tech Institute. (2016, September 1). DBT's approach to treating individuals at high risk for suicide. Retrieved February 2026, from https://behavioraltech.org/dbt-approach-treating-individuals-high-risk-suicide/
Madere, J., & Coy, D. M. (2024). Standards of care and ethical challenges for using EMDR therapy in the treatment of complex trauma and dissociation. International Society for the Study of Trauma and Dissociation Center for Advanced Studies. https://cfas.isst-d.org/content/standards-care-and-ethical-challenges-using-emdr-therapy-treatment-complex-trauma-and
Madere, J., & Coy, D. M. (2025, March 7). Ethics and EMDR therapy. EMDR International Association. https://www.emdria.org/blog/ethics-and-emdr-therapy/
SimplePractice. (2023). Therapist burnout report: What's behind the mental health workforce crisis. Retrieved February 2026, from https://www.simplepractice.com/blog/therapist-burnout-report/
TTI Internal Resources
Trauma Therapist Institute. (n.d.). EMDR and complex PTSD. Retrieved February 2026, from https://www.traumatherapistinstitute.com/emdr-and-complex-ptsd
Trauma Therapist Institute. (n.d.). EMDR and somatic therapy. Retrieved February 2026, from https://www.traumatherapistinstitute.com/EMDR-and-Somatic-Therapy
Trauma Therapist Institute. (n.d.). EMDR vs. somatic experiencing. Retrieved February 2026, from https://www.traumatherapistinstitute.com/blog/EMDR-vs-Somatic-Experiencing
Trauma Therapist Institute. (n.d.). Polyvagal theory and EMDR. Retrieved February 2026, from https://www.traumatherapistinstitute.com/Polyvagal-Theory-and-EMDR
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.